[ad_1]
Yves right here. I need to confess to not having been sufficiently imaginative. Sometimes, we’ve featured posts from Well being Care Renewal on the appreciable misuse of digital well being data, or EHRs. They supplied the promise of way more correct, persistently documented, and straightforward to look at affected person histories. As a substitute, they had been optimized for billing, not affected person care. They’ve grow to be a time sink for docs and may degrade affected person care by forcing the physician to focus on pages of tick the field varieties on the expense of analyzing the case earlier than him.
Right here we be taught of a brand new offense: that hospitals are enjoying definitional video games in order to withhold data from sufferers and the attorneys that symbolize them, notably MD notes which might present adjustments in affected person situation versus medical interventions. What’s worse, as this submit exhibits, an in depth letter to Mickey Tripathi, the Well being and Human Providers official accountable for well being data know-how, acquired a brush off from a minion.
I encourage involved readers to jot down Tripathi and cc their Congresscritters. Merely a brief observe asking about his lack of curiosity on this violation of affected person rights within the face of HIPAA complaints being ineffective may stir the pot. On points the place bureaucrats count on nobody to be watching, it takes surprisingly few letters to get them nervous.
By Informatics MD. Initially printed at Health Care Renewal
This alternate I had with the Workplace of the Nationwide Coordinator for Well being IT (ONC) at HHS must be of curiosity. It comes from my now-12-plus years expertise as forensic knowledgeable in EHR-related litigation:
———————–
April 19, 2023
Micky Tripathi, Ph.D., M.P.P.
Nationwide Coordinator for Well being Info Know-how
Well being and Human Providers
Washington, DC
Expensive Dr. Tripathi,
I’m a medical informatics specialist, former Yale NIH postdoctoral fellow 1992-94 after which college on the Yale Heart for Medical Informatics. I’m concerned in medico-legal EHR forensics lately.
Being concerned as an knowledgeable in numerous authorized issues presently the place discovery of digital data, audit trails and observe modifications has been ongoing for as much as a decade on account of misconceptions, decide confusion, and semantic abuses by the hospital sector has introduced me to jot down to you.
I’m writing to you relating to a problem I feel ONC must remark upon and make clear nationally. The problem considerations EHR data blocking by quite a few hospitals and attorneys.
I’ve skilled many examples the place hospitals have arbitrarily outlined their “designated report units” to not embrace observe modifications, and precise observe entry instances, which within the paper world had been an immutable a part of the paper report. (The precise entry instances had been mirrored within the observe sequence within the paper charts if not written explicitly by authors.) It must be famous that hospitals are taking important liberties in defining the contents of the DRS in order that they mirror the identical exceptions of the “authorized medical report” when responding to affected person requests for his or her full medical report.
The hospitals then don’t produce observe modifications and precise observe entry instances to sufferers on digital report requests, and oftentimes resist requests from their authorized representatives. I, actually, know of numerous circumstances the place this manufacturing failure has been ongoing for years, inflicting important authorized expense in courtroom battles to acquire this data and the place justice is thus delayed … or denied.
These actors appear to imagine that digital data cut back sufferers’ rights to this data in comparison with sufferers’ rights with paper data (relating to data that was inseparable from paper data), and that sufferers and their representatives must be blocked from receiving it in digital report manufacturing.
I feel it’s self-evident that observe adjustments and modifications in paper data are an immutable a part of that paper report and have to be produced to sufferers or the representatives as a part of the medical data. Eradicating, altering or withholding observe adjustments and modifications in paper data could be unquestionably deceptive in addition to improper spoliation of the data.
In paper data, observe corrections by means of cross-out and person correction/annotation don’t flip the unique feedback into metadata. They continue to be a part of the first data. Neither do observe modifications in digital data rework the unique observe into metadata; the modifications stay a part of the first data. Going digital mustn’t change affected person’s rights to this data.
Nevertheless, in digital data observe adjustments are often not proven on the report printout, however solely in an audit path or particular report. Hospitals keep that such report adjustments together with timing of medical report entries are metadata and/or a part of an audit path, and thus not topic to manufacturing on strange report requests primarily based on their “designated report set” definitions. Manufacturing of this data can be usually resisted on request of sufferers’ authorized representatives, requiring a lot authorized argument, educating judges on the problems, motions to compel, and wasted time and courtroom sources.
The precise entry order of the notes themselves are additionally an immutable a part of paper data, whereas in digital data a user-selected show date and time are sometimes used to order the chronologic print out of notes, obscuring the precise sequence of observe entry. The precise report instances oftentimes aren’t proven in the usual report printout.
Thus, with out the sufferers’ rights to obtain such knowledge with an ordinary data request, medical care notes and entries can undetectably be entered late – hours, days, weeks or longer after scientific occasions – and sufferers and their representatives are misled about when such notes and entries had been really made.
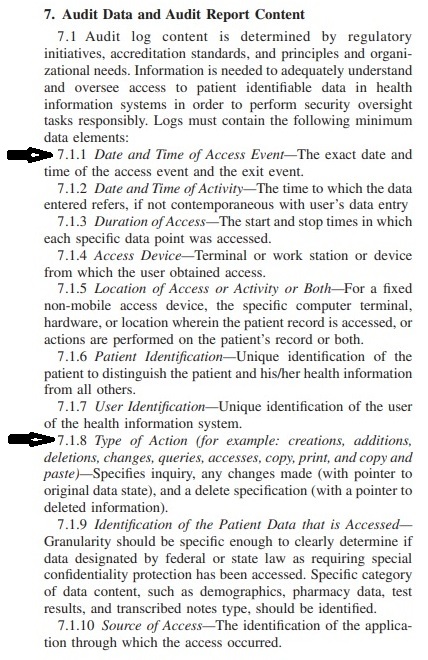
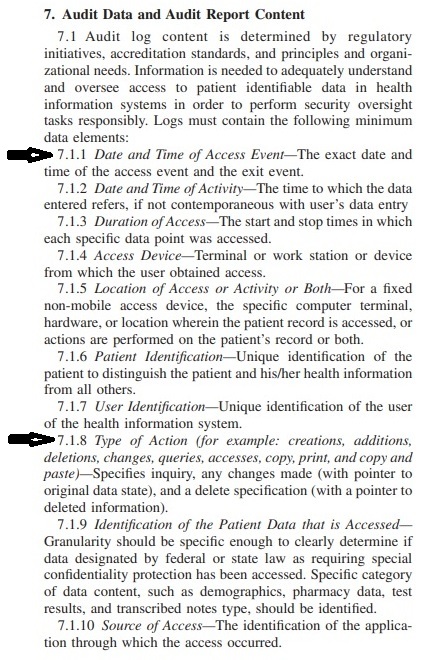
The prevalent customary utilized by HHS for audit trails in healthcare data programs, ASTM E2147-18, mandates that licensed EHRs seize this data – previous variations of notes and id of who modified them and when, and precise instances of entry- of their audit trails. However that is being ignored by many healthcare entities in affected person report requests.
ASTM E2147-18 Audit path obligatory content material (click on to enlarge)
My query is that this. Does ONC imagine that the transfer to digital data from paper data reduces affected person’s rights to data comparable to observe modifications and observe entry instances?
If that’s the case, why?
If not, a nationwide clarification is required from ONC to stop this drawback from persevering with to happen.
I’ve additionally grow to be conscious of a member hospital of a bigger nationwide hospital chain’s protection workforce making the next assertion about an EMR report the place the forensic proof is simple and exhibits, amongst different points, deletion of an vital observe, however the place the protection states to the courtroom that the chart is ok. The case is of a mom whose little one was grievously injured at start. This assertion was filed with the courtroom this month:
“… it’s this Defendant’s place that the medical data are topic to the enterprise report exception and due to this fact are authenticated by advantage of the exception.”
This, after all, is a preposterous place relating to authenticity of digital data, utterly ignoring ASTM E2147-18 definitions on authentication and what that entails, however many judges have no idea higher.
This can not proceed.
Sincerely,
S. Silverstein
—————————————
A response got here just a few days later:
From: Marchesini, Kathryn (OS/ONC) <Kathryn.Marchesini@hhs.gov>
Date: Mon, Apr 24, 2023 at 3:35 PM
Topic: Re: Letter to ONC DirectorTripathi hooked up relating to authorized points and EMR data blocking
Cc: Tripathi, Micky (OS/ONC) <Micky.Tripathi@hhs.gov>
Dr. Silverstein:
Thanks for bringing this matter to our consideration. From the knowledge you shared with ONC, it appears your questions and considerations relate to the HIPAA Privateness Rule
Should you imagine {that a} HIPAA-covered entity or its enterprise affiliate violated your (or another person’s) well being data privateness rights or dedicated one other violation of the HIPAA Privateness, Safety, or Breach Notification Guidelines, chances are you’ll file a complaint with the HHS Workplace for Civil Rights (OCR).
Variety regards,
Kathryn
Kathryn Marchesini, JD, CISSP
Chief Privateness Officer
Workplace of the Nationwide Coordinator for Well being IT (ONC)
U.S. Division of Well being and Human Providers
I responded again:
From: S Silverstein
Date: Tue, Apr 25, 2023 at 12:24 PM
Topic: Re: Letter to ONC DirectorTripathi hooked up relating to authorized points and EMR data blocking
To: Marchesini, Kathryn (OS/ONC) <Kathryn.Marchesini@hhs.gov>
Cc: Tripathi, Micky (OS/ONC) <Micky.Tripathi@hhs.gov>
Expensive Ms Marchesini,
Thanks to your response.
I’m conscious of the hyperlink for submitting complaints with the HHS OCR.
The issue I’m describing, nevertheless, is a bit totally different. It’s way more pervasive than merely the circumstances I’ve been concerned in, and has a simple resolution.
What has been ongoing since I began forensics work in 2010 is systematic, ongoing, pervasive discovery abuse and even fraud by a mess of hospitals and nursing houses in a number of states throughout this nation. My colleagues report the identical phenomena.
I’ve personally written dozens of affidavits within the litigation battles for manufacturing of full data, audit trails and observe modification histories. I’ve watched delay after delay after delay, wasteful of courtroom sources and cash. These battles must be utterly pointless.
It’s a nationwide drawback.
An answer is clarification from ONC and HHS on hospitals obligations for EMR manufacturing, that may additionally educate the judiciary who might be swayed by essentially the most absurd arguments for a healthcare group’s failure to supply.
As an example, one other preposterous declare I’ve heard on quite a few events in litigation is that the 2010 model of 45 CFR 170.210 didn’t particularly command hospitals to retailer or retain observe model histories, solely person actions. Due to this fact, previous to the 2012 model (which referred to as for adherence to ASTM E2147), hospitals declare they got an open license to not retailer or delete the prior variations of altered notes, flip off that function of their EHRs, or purchase EHR know-how that lacked the aptitude.
Judges are typically unknowledgeable about these issues.
I hope we are able to agree that, relating to the 2010 model of 45 CFR 170.210 “Requirements for well being data know-how to guard digital well being data created, maintained, and exchanged”, the said key challenge is:
Safety of well being data and digital medical report integrity.
The 2010 model of 45 CFR 170.210 doesn’t explicitly state that audit trails should comprise a observe modification historical past.
Nevertheless, this regulation couldn’t fairly be interpreted as overriding paper data requirements of care that decision for not obscuring or obliterating authentic variations of altered notes or paperwork, and giving license to hospitals to capriciously and freely obliterate earlier variations of modified notes or paperwork. That’s not safety, that’s observe destruction.
Such an interpretation is absurd, however is submitted with a straight face in courtroom.
The 2010 model of 170.210 additionally couldn’t fairly be interpreted as overriding earlier well being care data system federal rules from the exact same Dept. of Well being and Human Providers that regulates hospital digital medical data programs.
For instance in pharma – 21 CFR half 11 of 1997 entitled “Meals and Drug Administration, Division of Well being and Human Providers, ELECTRONIC RECORDS; ELECTRONIC SIGNATURES”, subpart B,
- 11.10 Controls for closed programs,
mandates at (e):
(e) Use of safe, computer-generated, time-stamped audit trails to independently report the date and time of operator entries and actions that create, modify, or delete digital data. Report adjustments shall not obscure beforehand recorded data. Such audit path documentation shall be retained for a interval a minimum of so long as that required for the topic digital data and shall be accessible for company overview and copying.
Lastly, in 2012 an replace to 170.210 did particularly name for digital medical report audit trails in hospitals to stick to the ASTM E2147-09 well being care audit path customary of 2009. That customary specifies that in audit trails, pointers have to be maintained to earlier variations of altered data.
170.210 was later up to date to the ASTM E2147-18 2018 model, which about audit path content material says the identical because the 2009 model.
Clearly HHS’s intent was to take care of the identical customary of care as in paper report holding, and to not give license to hospitals to obliterate or destroy earlier variations of altered notes or paperwork.
Easy statements from ONC clarifying hospital obligations with regard to manufacturing of medical data, observe modifications, and different audit knowledge not being non-obligatory nor topic to debate, might assist resolve the state of affairs that’s ongoing for a few years. Discovery resistance is often identified to EHR forensics specialists and trial attorneys.
The bills to combat it come from injured sufferers’ or deceased sufferers’ household’s potential compensation – that’s, when justice is just not denied them by means of manipulation of the EHR discovery course of.
Sincerely,
- Silverstein—————————————
I await an extra response.
— SS

[ad_2]
